Author: Dr. Riccardo Rosa
Neck pain is a very common disease among the adult population of developed countries and contributes significantly to the demand for medical services and the economic burden of absence from work. Population-based studies suggest a lifetime prevalence of over 70% and a point prevalence between 12 and 34% [1].
Work-related neck disorders are common among office workers, especially those who are intensive computer users [2]. The average time of use of computers is now constantly increasing. In fact, devices such as PCs, tablets and smartphones are increasingly used both for work and during leisure time, thus increasing the risk of developing cervical problems.
The guidelines recommend the assessment of active and passive range of motion (ROM) so that the level of impairment of body function can be identified, the appropriate treatment path can be set and changes monitored over time. Within the rehabilitation process of acute and chronic issues, the use of an exercise program for the ROM of the neck and the strengthening of both the scapulo-thoracic and upper limbs is also recommended [3].
Anamnesis
30-year-old girl, partner of a graphics and advertising studio, new mother. Not practicing physical activity. For 2 months she has felt paresthesia (tingling) in the hands, especially on the right side, associated with neck stiffness, and intermittent pain related to movements. The patient complains of difficulty in cervical movement and a feeling of heaviness from the neck to the hand. In the last period, the frequency of tingling and pain have intensified due to the time spent working sitting in front of the computer. The patient is rather worried about her symptoms as they are limiting in some household and daughter management activities.
Assessment
During the assessment, the following tests are administered:
- Cervical ROM test with the support of baiobit
It is performed on the three anatomical planes, repeating each movement 3 times, showing the following results (Figure 1):
- left rotation 62°, right rotation 71° with 5/10 VAS pain
- extension 49°, flexion 51° without pain VAS 0/0
- left lateral flexion 34°, right lateral flexion 48° with 4/10 VAS pain
This shows an inhomogeneous active range of motion in the sagittal and coronal planes, with various differences between the execution speeds. The rotational and lateroflexion movements trigger the patient's symptom.
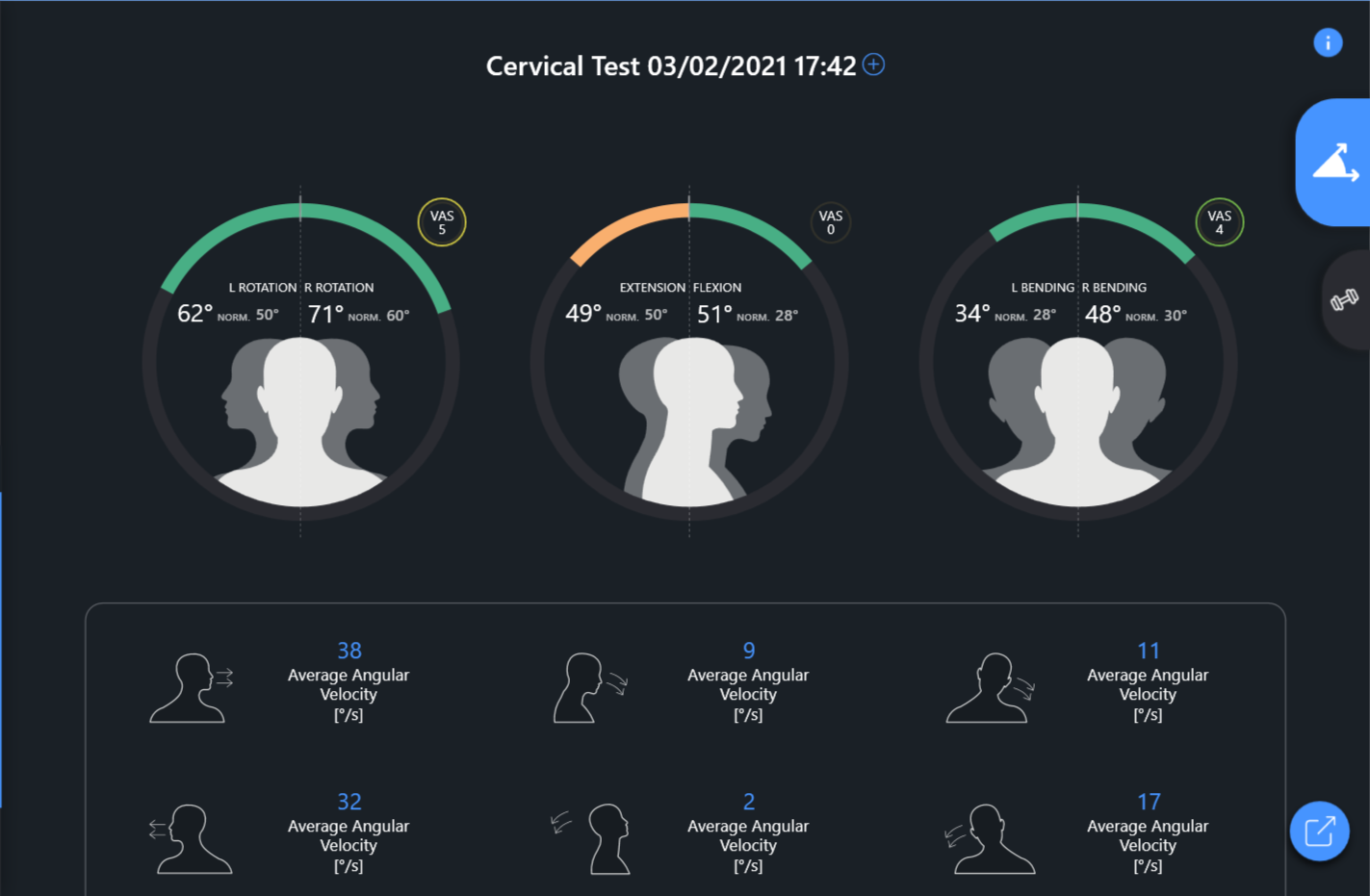
Figure1 - Initial Cervical Range Of Motion Test
• Differentiation test to exclude the presence of serious problems and neurological deficits in progress, which would otherwise require a specialist medical examination
• Test for the evaluation of neurodynamic sensitivity
• Provocative palpation test of nerve and soft tissues, which confirms the presence of numerous hypersensitive and provocative myofascial areas associated with dysfunctions and hypersensitivity of the corresponding joint segments at the level of the lower cervical (C3-C4-C5), at the cervico-thoracic level ( C7-T1-T2) with involvement of the first rib (K1).
In general, the evaluation performed indicates the presence of muscle-joint movement dysfunctions at the cervical and thoraco-costal level, with symptoms triggered by nociceptive mechanisms.
Rehabilitation Program
A rehabilitation program of 3 sessions is set up approximately 5 days apart, where the following are performed:
• cervical, thoracic and first rib HVLA joint manipulation techniques
• manual neuro-muscular techniques to improve ROM
• exercises for the improvement of regional mobility combined with neurodynamics, to be performed directly at home. The exercise sheet is processed through the use of the baiobit software (Figure 2)
Figure 2: Home exercises
Results
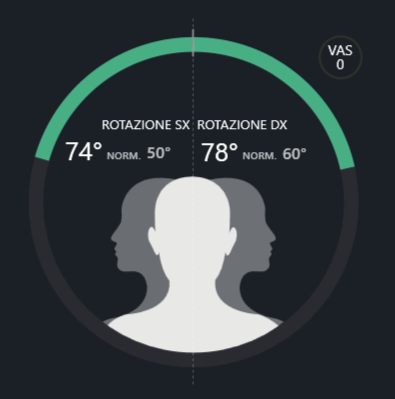
At the end of the third session a re-evaluation is performed, in particular the ROM evaluation with the support of baiobit is performed again for an objective measurement of the outcomes. An improvement in the ROM in flexion and extension emerges, in addition to the disappearance of painful symptoms and tingling (Figure 3).
| Initial assessment | Final assessment |
R/L ROTATION | 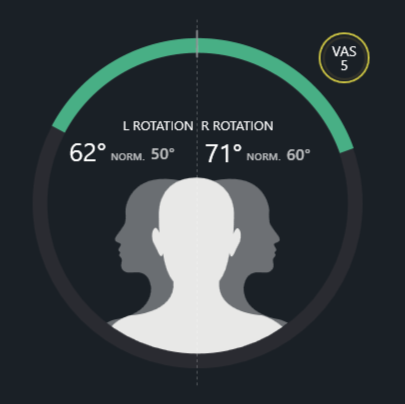
| 
|
FLEX-EXTENSION | 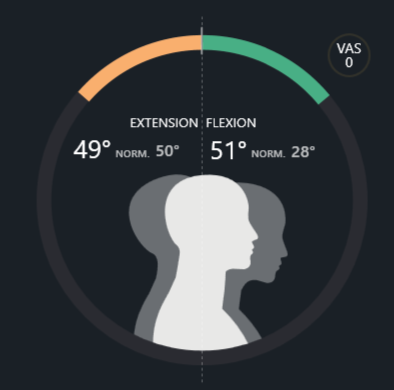 | 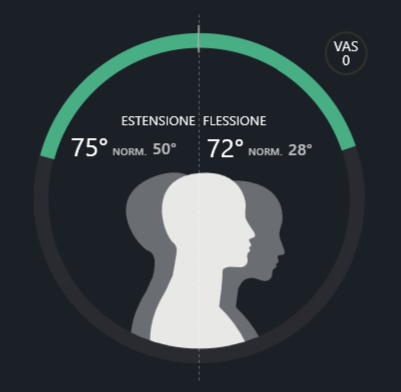 |
R/L LATERAL FLEXION | 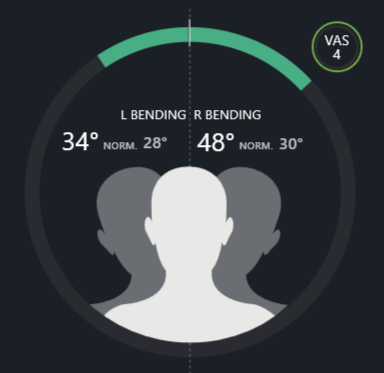 | 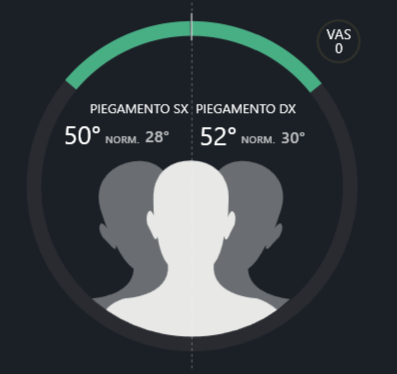 |
Figure3: final cervical Range Of Motion test
In addition to the measurements performed, the patient is shown the evolution before and after the rehabilitation process so that she can fully appreciate the improvements obtained. Here are the results:
• right rotation 9% improvement
• left rotation improvement of 19%
• downturn improvement of 41%
• 53% improvement extension
• right lateral flexion 8% improvement
• left lateral flexion improvement of 47%
• disappearance of the painful symptoms on the 3 levels of movement
Bibliografia
[1] Buckle, P. W., & Devereux, J. J. (2002). The nature of work-related neck and upper limb musculoskeletal disorders. Applied ergonomics, 33(3), 207-217.
[2] Jensen, C. (2003). Development of neck and hand-wrist symptoms in relation to duration of computer use at work. Scandinavian journal of work, environment & health, 197-205.
[3] Blanpied, P. R., Gross, A. R., Elliott, J. M., Devaney, L. L., Clewley, D., Walton, D. M., ... & Robertson, E. K. (2017). Clinical practice guidelines linked to the International classification of functioning, disability and health from the orthopaedic section of the American physical therapy association. Journal of Orthopaedic and Sports Physical Therapy, 47(7), A1-A83.